
 AstraZeneca covishield claimed its rare side effect,thrombotic thrombocytopenic syndrome. A critical condition characterized by the formation of blood clots alongside reduced platelet levels.
AstraZeneca covishield claimed its rare side effect,thrombotic thrombocytopenic syndrome. A critical condition characterized by the formation of blood clots alongside reduced platelet levels.
Patient Education and Awareness plays a significant role in curbing down mortalities.
Thrombotic Thrombocytopenia Syndrome (TTS), also known as “vaccine-induced immune thrombotic thrombocytopenia (VITT),” is a rare condition that emerges following an immune response to the vaccine.
Thrombosis and thrombocytopenia, both cycles happen simultaneously, an autoantibody called platelet factor 4 ,(PF4) antibody, activated the platelets to form clot causing thrombosis, platelet get consumed and thus lowering their number causing thrombocytopenia as a part of the condition.
The blood clots can occur in any part of the body, including:
- The brain (referred to as cerebral venous sinus thrombosis, or CVST)
- The abdomen (known as splanchnic vein thrombosis)
- The lungs (referred to as pulmonary embolism)
- Limb veins (referred to as deep vein thrombosis, or DVT)
- Arteries (known as arterial thrombosis)
A strict no to heparin
Vaccine-Induced Thrombotic Thrombocytopenia (VITT), antibodies form against PF4.
This triggers platelet activation, thrombosis, and decreases platelet count through thrombocytopenia.
Heparin has dual mechanism of action, it binds to antithrombin III as well as has binding for PF4.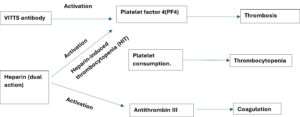
Antithrombin binding cause anticoagulant effect but binding to PF4 trigger an immune response producing antibodies against the complex and causing heparin induced thrombocytopenia leading to platelet activation, thrombosis, increase consumption of platelets and ultimately lowering the count.
Heparin exacerbates this condition by further activating platelets and contributing to thrombocytopenia.